
Abstract
Phenotypic age acceleration (PhenoAgeAccel) is a novel biological indicator estimates an individual’s mortality risk. The primary aim of this study was to evaluate the association between PhenoAge and PhenoAgeAccel with incident cardiovascular diseases (CVD) in the UK Biobank cohort. We analyzed data from 114,517 UK Biobank participants free of CVD history at baseline. PhenoAgeAccel of was obtained by regressing PhenoAge on chronological age (ChronoAge). We applied a Cox regression model with time-dependent variables to assess the association between PhenoAgeAccel and incident CVD. The predictive value of PhenoAge and PhenoAgeAccel was evaluated with reference to the Framingham Risk Score (FRS) model using Kaplan-Meier curves, receiver operating characteristic curves (AUC), and Harrel’s C-index. The positive PhenoAgeAccel comprised of 36.5% of the cohort. The mean ChronoAge and PhenoAge of participants in the positive PhenoAgeAccel group was 57.5 years and 61.7 years, respectively. The mean ChronoAge and PhenoAge of participants in the negative PhenoAgeAccel group was 56.1 years and 52.5 years, respectively. Incident CVD occurred at a higher rate in the positive PhenoAgeAccel group (44.8% vs. 33.1%) at a comparatively shorter period (11.2 years vs. 12.4 years). The AUC of PhenoAge in predicting incident CVD was lower than the FRS but higher than ChronoAge (69.3% vs. 70.9% vs. 68.1%, respectively). Discriminative performance was assessed using Harrell’s C-index. The model including established cardiovascular risk factors yielded a C-index of 0.670, compared to 0.674 for the model incorporating PhenoAgeAccel (difference = 0.0049, p < 0.001). Separately, the Framingham Risk Score (FRS) model achieved a higher C-index of 0.697 versus 0.674 for the PhenoAgeAccel model (difference = 0.022, p < 0.001). Kaplein-Meier survival patterns of the positive PhenoAgeAccel group was similar to the high-risk group of FRS level. At time points year 4, 8, 12, and 16, the freedom-from-CVD probability for positive PhenoAgeAccel groups versus FRS high risk groups were 86.2% vs. 85.7%, 72.6% vs. 71.1%, 60.0% vs. 57.4%, and 54.8% vs. 51.7% respectively. Positive PhenoAgeAccel was associated with higher 10-year CVD risk, suggesting its potential as an adjunct in CVD risk assessment. PhenoAge, by incorporating biological aging markers, may offer more nuanced risk insights compared to ChronoAge. These findings are primarily applicable to men, given the male predominance in the cohort, and should be interpreted with caution for women.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality worldwide1. In the United States, CVD prevalence increases with age, ranging from 1.4 to 13.8% among adults aged 20–39 years, 9.2–57.6% in those aged 40–59, 19.6–77.8% for ages 60–79, and 32.8–85.9% in individuals aged ≥ 80.2 To mitigate this growing burden, global strategies focus on primary prevention and risk assessment tools, such as the Framingham Risk Score (FRS), Pooled Cohort Equations, and Systematic Coronary Risk Evaluation2,3. Among these, age is a key predictive factor.
Ageing is characterized by a progressive decline in physiological function, increasing vulnerability to chronic conditions4. Chronological age (ChronoAge), the number of years since birth, is a major non-modifiable CVD risk factor5. However, individuals with the same ChronoAge often show varying susceptibility to disease and mortality, suggesting that ChronoAge may not adequately capture biological ageing. To address this, alternative measures based on clinical biomarkers have emerged6. One such metric, phenotypic age (PhenoAge), estimates biological ageing and has shown utility in predicting disease risk across diverse populations7. A positive PhenoAge acceleration (PhenoAgeAccel)—when PhenoAge exceeds ChronoAge—indicates faster biological ageing. PhenoAgeAccel has been linked to environmental exposures, chronic diseases, autoimmune and mental health conditions, and lifestyle factors8,9,10,11. Notably, the American Heart Association Scientific Sessions 2023 reported an association between positive PhenoAgeAccel and poorer cardiovascular health12. However, its role in predicting incident CVD remains unexplored.
This study aimed to examine the associations between PhenoAge, PhenoAgeAccel, and incident CVD using data from the UK Biobank, and to evaluate their predictive value for 10-year CVD risk in comparison to the FRS.
Methods
Study population and design
The UK Biobank is a prospective cohort that recruited approximately > 500,000 adults from the United Kingdom between 2006 and 2010 from 22 assessment centers. The study design and data collection methods used in the UK Biobank has been previously reported. The UK Biobank has institutional review board approval from the Northwest Multicenter Research Ethics Committee, and all participants provided written informed consent. Secondary use of data for present analysis was approved by the Fudan University Pudong Medical Center Institutional Review Board. The study was conducted in accordance with relevant guidelines, including the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline and regulations13.
Selection criteria
Participants with pre-existing cardiovascular disease (CVD) at baseline or those diagnosed with incident CVD within one year of recruitment were excluded. Individuals with chronic kidney disease were also excluded due to their elevated risk of both ischemic and hemorrhagic events. Those with a prior cancer diagnosis were omitted to avoid confounding overall survival analyses. Missing baseline data were not imputed.
PhenoAge and phenoageaccel
PhenoAge was developed based on mortality scores from the Gompertz proportional hazard model on ChronoAge and 9 multisystem clinical chemistry biomarkers (i.e. albumin, alkaline phosphatase, creatinine, glucose, C-reactive protein, lymphocyte percentage, mean cell volume, red cell distribution width, and white blood cell count) to predict all-cause mortality using the National Health and Nutrition Examination Surgery (NHANES) III data7. PhenoAgeAccel is the difference between one’s PhenoAge and ChronoAge. A higher PhenoAgeAccel (> 0) indicates faster biological aging.
CVD risk factors and risk assessment
ChronoAge and CVD risk factors for participants were collected from baseline. The following baseline variables were considered: blood pressure levels (systolic and diastolic), smoking history (includes active and past smokers), body mass index (BMI), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides, documented prescription of CVD preventive drugs (includes antihypertensives, cholesterol-lowering drugs, and insulin), and diabetes history. The FRS was calculated based on 6 coronary risk factors including ChronoAge, gender, TC, HDL-C, systolic blood pressure, and smoking habits14. Ten-year risk in percentage were calculated by total points and the absolute CVD risk percentage over 10 years was classified as low risk (< 10%), intermediate risk (10–20%), and high risk (> 20%).
Outcome ascertainment
The outcome of this study was incident CVD, which were recorded using the International Classification of Diseases 10th Revision code and defined as I20-25 for ischemic heart disease, I46-52 for cardiac arrest, rhythm disorders, and heart failure, I60-69 for cerebrovascular disease, I70 for atherosclerosis. Outcomes excluded were I51.4 for unspecified myocarditis, I60 for subarachnoid hemorrhage, I62 for subdural hemorrhage, I67.1 for cerebral aneurysm, I68.2 for cerebral arteritis, and I67.5 for moyamoya disease. The UK Biobank Outcome Adjudication Group, in conjunction with clinical experts, developed and validated algorithms based on lists of clinical codes to ascertain a range of health outcomes (https://biobank.ndph.ox.ac.uk/showcase/showcase/docs/alg_outcome_main.pdf), including myocardial infarction and stroke, which were used in this study. Censoring was defined as the time of death, withdrawal from the study or end of follow-up, whichever came first. This study was conducted using the UK Biobank resource, application 103,791.
Statistical analysis
All statistical analyses were conducted using R Studio (Version 2023.12.1 + 402, Posit Software, PBC). Subgroup analyses (i.e. by gender, diagnosis of diabetes, positive or negative PhenoAgeAccel, 10-year CVD risk based on FRS groups, and number of CVD preventive drugs prescribed) were performed. The student t test and χ15 tests were used to compare differences in quantitative (i.e. mean ± standard deviation) and qualitative (i.e. number [%]) data, respectively. Continuous variables of normal distribution were evaluated using the analysis of variance (ANOVA) test, whereas the Kruskal-Wallis test was used for non-normally distributed data. The relationship between PhenoAge and incident CVD was assessed using biserial correlation. Cox proportional hazards regression models were used to assess the associations of PhenoAgeAccel with incident CVD, as well as estimate hazard ratio (HR) and 95% confidence intervals (CI) with adjustment for ChronoAge, gender, smoking history, diabetes, use of CVD preventive drugs, and lipid levels. Harrell’s C-index was used to assess the discriminative performance of Cox proportional hazards models based on established CVD risk factors, PhenoAgeAccel, and the FRS. The Kaplan-Meier survival curve is plotted to compare CVD survival between PhenoAgeAccel groups. Area under receiver operative characteristic (ROC) curves (AUC) were obtained to estimate the sensitivity and specificity of PhenoAge towards incident CVD. A two-sided p value < 0.05 was considered to be statistically significant.
Results
Participants
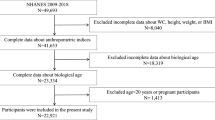
The final analysis included 114,517 participants. Figure 1 demonstrates the flowchart of participant selection and analytic construction. The cohort mainly comprised male participants (99.7%, n = 113,288) and the distribution of baseline characteristics is summarized in Table 1. A total of 42,782 (37.3%) participants had documented incident CVD diagnosed over a 12.0 ± 4.6 years follow-up duration.

Flow diagram showing the process of participant selection and analysis conducted.
Phenotypic ageing, phenoageaccel, and incident CVD
The mean ChronoAge and PhenoAge of participants in the positive PhenoAgeAccel group was 57.5 ± 8.1 years and 61.7 ± 9.9 years, respectively. The mean ChronoAge and PhenoAge of participants in the negative PhenoAgeAccel group was 56.1 ± 8.2 years and 52.5 ± 8.6 years, respectively. The percentage of patients with diabetes was notably higher in the positive PhenoAgeAccel group (11.6% vs. 3.1%). Incident CVD occurred at a higher rate in the positive PhenoAgeAccel group (44.8% vs. 33.1%) at a comparatively shorter period (11.2 ± 4.9 years vs. 12.4 ± 4.4 years). When distributed according to the FRS level, more than half of the participants of both positive and negative PhenoAgeAccel groups were at high risk (68.9% and 59.4%, respectively). Biserial correlation analysis showed a moderate positive correlation between PhenoAge and incident CVD (ρ = 0.322, 95% CI 0.317–0.327, p < 0.001).
Given the discrepancies in gender, a subgroup analysis between male and female patients were conducted (Table S1). Incident CVD was 1.7 times higher in the included females than males (64.4% vs. 37.3%). The mean PhenoAge of females was older than males (67.2 ± 12.9 years vs. 55.8 ± 10.1 years) and older than their ChronoAge (58.8 ± 7.2 years).
Nearly all included females were diagnosed with diabetes and all required CVD preventive drugs. Therefore, additional subgroup analysis was compared according to participant’s history of diabetes and CVD preventive drug numbers (Table S1). It was found that patients with diabetes had older mean PhenoAge than patients without diabetes (65.3 ± 11.3 years vs. 55.2 ± 9.7 years).
The AUC for ChronoAge, PhenoAge, PhenoAgeAccel, and FRS were 68.1% (68.5%, 41.4%), 69.3% (80.0%, 52.9%), 58.4% (58.9%, 58.0%), and 70.9% (73.6%, 43.1%), respectively (Fig. 2). The discriminative performance of multiple Cox models was compared using Harrell’s C-index. The model with established cardiovascular risk factors yielded a C-index of 0.670, while the model that included PhenoAgeAccel had a C-index of 0.674. The difference in C-indices was 0.0049 (p < 0.001). In a separate comparison, the FRS model showed a C-index of 0.697, compared to 0.674 for the PhenoAgeAccel model, with a difference of 0.022 (p < 0.001).

Receiver-operating characteristic curves for incident cardiovascular disease. (A) represents for chronological age; (B) represents for the Framingham Risk Scores; (C) for phenotypic age; and (D) for phenotypic age acceleration.
Table 2 presented the HR and 95% CIs of PhenoAge and PhenoAgeAccel on incident CVD. The associations remained robust after adjustment for potential CVD risk factors. In model 2, the multivariate adjusted HRs (95% CIs) for PhenoAge per year and PhenoAgeAccel were 1.023 (1.022–1.025, p < 0.001) and 1.222 (1.198–1.246, p < 0.001) respectively.
PhenoAgeAccel and FRS for 10-year CVD survival
Table 3 summarized the distribution of PhenoAgeAccel groups according to different FRS levels. Mean PhenoAges were slightly younger than the mean ChronoAge. There was an increase in participants with positive PhenoAgeAccel from low to high FRS levels. The incidence of CVD for low-, intermediate-, and high-risk groups were 10.8% (n = 1427), 23.2% (n = 6807), and 48.0% (n = 34528) respectively. The mean duration for CVD to occur was shorter in the high-risk group when compared to intermediate- and low-risk groups (11.0 ± 5.0 years vs. 13.3 ± 3.7 years vs. 14.3 ± 2.5 years). Kaplein-Meier survival patterns of the positive PhenoAgeAccel group was similar to the high-risk group of FRS level (Fig. 3). At time points year 4, 8, 12, and 16, the freedom-from-CVD probability for positive PhenoAgeAccel groups versus FRS high risk groups were 86.2% vs. 85.7%, 72.6% vs. 71.1%, 60.0% vs. 57.4%, and 54.8% vs. 51.7% respectively.

Kaplan-Meier curves for incident cardiovascular events in the (A) positive versus the negative PhenoAgeAccel groups; and (B) different risk levels based on the Framingham Risk Score.
Discussion
Several biological aging parameters have been linked to chronic diseases, including CVD. While previous studies briefly noted the association between PhenoAgeAccel and CVD, this study provides deeper insight into the relationship between PhenoAge, PhenoAgeAccel, and incident CVD, using a longitudinal analysis of 114,517 participants from the UK Biobank. We also compared these findings to the FRS as a reference.
Both higher PhenoAge and a positive PhenoAgeAccel were associated with increased CVD risk (adjusted HR 1.2, p < 0.001), reflected in the higher incidence (44.8% vs. 33.1%). These findings align with the understanding that individuals with faster biological aging may experience higher CVD risk. Although differences in PhenoAge between FRS categories were modest (0.3–2.2 years), individuals with negative PhenoAgeAccel accounted for ≥ 60% of each FRS risk category. However, the proportion of those with positive PhenoAgeAccel increased as FRS risk level rose, suggesting that PhenoAgeAccel could enhance the identification of individuals at elevated risk, refining predictions beyond traditional models like FRS.
When evaluating model discrimination, incorporating PhenoAgeAccel improved the C-index from 0.670 to 0.674 (p < 0.001) compared to models based solely on established cardiovascular risk factors. Although the FRS model demonstrated a higher C-index (0.697), the difference (0.022) was statistically significant (p < 0.001), reflecting the relative improvement offered by PhenoAgeAccel.
ChronoAge represents linear time, while biological age reflects physiological variation as captured through biochemical markers16. These markers are influenced by factors such as stress, diet, exercise, and sleep, which may introduce some short-term variability17,18,19. Unlike ChronoAge, which primarily reflects chronological time, PhenoAge incorporates additional markers of biological aging, which may enhance the predictive power of traditional risk models. To anchor our analysis, we compared PhenoAge with the well-established FRS model, which is widely used for predicting 10-year cardiovascular risk20,21. However, as previously noted, FRS has certain limitations, particularly in light of newer models like the pooled cohort Equations and SCORE2, which could provide additional insights22,23.
We explored the associations between gender, diabetes, and CVD preventive drug use with PhenoAge. Due to exclusion criteria, only 0.3% of participants in our cohort were women, all of whom required antihypertensives, cholesterol-lowering drugs, and insulin, resulting in significantly higher PhenoAge values than the male participants (67.2 vs. 55.8 years, p < 0.001). This limits the generalizability of the findings to women, reflecting the dataset’s structure, where UK Biobank participants are predominantly aged ≥ 45 years, naturally placing many at intermediate risk by default24. Additionally, analysis of CVD preventive medications revealed that participants using all three drug types had the highest CVD risk and PhenoAge, possibly reflecting confounding by indication or medication nonadherence, given the lack of detailed data on medication usage patterns in the UK Biobank.
Consistent with previous studies, diabetes was strongly linked to accelerated biological aging25,26. In our cohort, individuals with diabetes had PhenoAge values 10 years older than those without diabetes (65.3 vs. 55.2 years), while their ChronoAge was paradoxically lower (56.4 vs. 60.1 years). Among those with diabetes, 68.3% were in the positive PhenoAgeAccel group, with a CVD incidence rate 1.8 times higher than in those without diabetes (63.9% vs. 35.5%), highlighting the potential of PhenoAgeAccel as a marker for heightened risk in diabetic individuals. This suggests that combining PhenoAge with ChronoAge may offer superior predictive performance over ChronoAge alone, particularly in populations at high cardiovascular risk.
A major strength of this study is the large cohort size, providing robust statistical power. However, limitations include the underrepresentation of women, due to exclusion criteria such as prior ASCVD or cancer, conditions often diagnosed earlier in women. Additionally, the later onset of CVD in women and the baseline age range of the cohort likely contributed to selection bias27. To address sex differences, we included sex as a covariate in all adjusted models and conducted subgroup analyses by sex. However, results for women should be interpreted with caution due to the limited sample size. While comparison with newer models like SCORE2 would have been informative, the retrospective cohort design precluded regional risk stratification28. Furthermore, incomplete follow-up data limited our ability to analyze longitudinal changes in PhenoAge, so only baseline values were used.
Despite these limitations, our findings suggest that PhenoAge has strong potential as an adjunct in cardiovascular risk stratification. When incorporated alongside traditional risk factors, such as ChronoAge, PhenoAge may improve personalized risk assessments by capturing more comprehensive biological aging signals. Unlike ChronoAge, which solely reflects chronological time, PhenoAge integrates physiological and biochemical markers, thus offering a more nuanced understanding of an individual’s cardiovascular risk. While PhenoAge and PhenoAgeAccel should not replace traditional risk factors, they can be valuable components in a broader, more dynamic model of CVD risk prediction. Future research should focus on evaluating how PhenoAge can track treatment effects, monitor risk over time, and be integrated into dynamic, multifactorial models. Moreover, incorporating PhenoAge into electronic health records, alongside emerging tools like epigenetic clocks and AI-driven prediction models, could significantly enhance CVD risk prediction and further support precision medicine in cardiovascular care.
Data availability
The data that supported the findings of this study are available from the UK Biobank (https://www.ukbiobank.ac.uk/) and the corresponding author (J.D.T.) upon reasonable request.
References
Vaduganathan, M., Mensah, G. A., Turco, J. V., Fuster, V. & Roth, G. A. The global burden of cardiovascular diseases and risk: A compass for future health. J. Am. Coll. Cardiol. 80 (25), 2361–2371 (2022).
Mendis, S., Graham, I. & Narula, J. Addressing the global burden of cardiovascular diseases; need for scalable and sustainable frameworks. Glob Heart. 17 (1), 48 (2022).
Sofogianni, A., Stalikas, N., Antza, C. & Tziomalos, K. Cardiovascular risk prediction models and scores in the era of personalized medicine. J. Pers. Med. 12 (7), 1180 (2022).
Ciumărnean, L. et al. Cardiovascular risk factors and physical activity for the prevention of cardiovascular diseases in the elderly. Int. J. Environ. Res. Public. Health. 19 (1), 207 (2021).
Damluji, A. A. et al. Chronological vs biological age in interventional cardiology: A comprehensive approach to care for older adults: JACC family series. JACC cardiovasc interv. 6 (2024).
Rutledge, J., Oh, H. & Wyss-Coray, T. Measuring biological age using omics data. Nat. Rev. Genet. 23 (12), 715–727 (2022).
Liu, Z. et al. A new aging measure captures morbidity and mortality risk across diverse subpopulations from NHANES IV: A cohort study [published correction appears in PLoS med. 2019;16(2):e1002760]. PLoS Med. 15 (12), e1002718 (2018).
Wang, T. et al. Associations of combined phenotypic ageing and genetic risk with incidence of chronic respiratory diseases in the UK biobank: a prospective cohort study. Eur. Respir J. 63 (2), 2301720 (2024).
Duan, S., Wu, Y., Zhu, J., Wang, X. & Fang, Y. Associations of polycyclic aromatic hydrocarbons mixtures with cardiovascular diseases mortality and all-cause mortality and the mediation role of phenotypic ageing: A time-to-event analysis. Environ Int. 29 https://doi.org/10.1016/j.envint.2024.108616 (2024).
Ori, A. P. S. et al. Meta-analysis of epigenetic aging in schizophrenia reveals multifaceted relationships with age, sex, illness duration, and polygenic risk. Clin. Epigenet.. 16 (1), 53 (2024).
You, Y. et al. Inverted U-shaped relationship between sleep duration and phenotypic age in US adults: a population-based study. Sci. Rep. 14 (1), 6247 (2024).
Following. ‘Life’s Essential 8’ Checklist May Slow Biological Aging by 6 Years. American Heart Association, 6 newsroom.Nov. (accessed 24 Apr 2024, 2023). https://newsroom.heart.org/news/following-lifes-essential-8-checklist-may-slow-biological-aging-by-6-years#:~:text=Instead%20of%20a%20calendar%20to,inflammation%20and%20organ%20function%20
von Elm, E. et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335 (7624), 806–808 (2007).
Sohn, C., Kim, J. & Bae, W. The Framingham risk score, diet, and inflammatory markers in Korean men with metabolic syndrome. Nutr. Res. Pract. 6 (3), 246–253 (2012).
Tsao, C. W. et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association [published correction appears in Circulation. 2023;147(8):e622]. Circulation. 147 (8), e93-e621 (2023).
Bafei, S. E. C. & Shen, C. Biomarkers selection and mathematical modeling in biological age Estimation. Npj Aging. 9, 13 (2023).
Galkin, F. et al. Psychological factors substantially contribute to biological aging: evidence from the aging rate in Chinese older adults. Aging (Albany NY). 14 (18), 7206–7222 (2022).
Ho, E., Qualls, C. & Villareal, D. T. Effect of diet, exercise, or both on biological age and healthy aging in older adults with obesity: secondary analysis of a randomized controlled trial. J. Nutr. Health Aging. 26 (6), 552–557 (2022).
Wang, M. et al. Association between sleep traits and biological aging risk: a Mendelian randomization study based on 157 227 cases and 179 332 controls. Sleep 47 (3), zsad299 (2024).
Mahmood, S. S., Levy, D., Vasan, R. S. & Wang, T. J. The Framingham heart study and the epidemiology of cardiovascular disease: a historical perspective. Lancet 383 (9921), 999–1008 (2014).
Urbut, S. M. et al. MSGene: a multistate model using genetic risk and the electronic health record applied to lifetime risk of coronary artery disease. Nat. Commun. 15 (1), 4884 (2024).
Brindle, P. et al. Predictive accuracy of the Framingham coronary risk score in British men: prospective cohort study. BMJ 327 (7426), 1267 (2003).
Talha, I., Elkhoudri, N. & Hilali, A. Major limitations of cardiovascular risk scores. Cardiovasc. Ther. 2024, 4133365 (2024).
Maas, A. H. & Appelman, Y. E. Gender differences in coronary heart disease. Neth. Heart J. 18 (12), 598–602 (2010).
Bahour, N. et al. Diabetes mellitus correlates with increased biological age as indicated by clinical biomarkers. Geroscience 44 (1), 415–427 (2022).
Ryder, J. R. et al. Accelerated early vascular aging among adolescents with obesity and/or type 2 diabetes mellitus. J. Am. Heart Assoc. 9 (10), e014891 (2020).
Ko, D. T. et al. Calibration and discrimination of the Framingham risk score and the pooled cohort equations. CMAJ 192 (17), E442–E449 (2020).
Graham, I. M. et al. Systematic coronary risk evaluation (SCORE): JACC focus seminar 4/8. J. Am. Coll. Cardiol. 77 (24), 3046–3057 (2021).
Acknowledgements
Ethics ApprovalThe UK Biobank has institutional review board approval from the Northwest Multicenter Research Ethics Committee, and all participants provided written informed consent. Secondary use of data for present analysis was approved by the Fudan University Pudong Medical Center Institutional Review Board.
Funding
This study received funding from the Shanghai Academy of Educational Sciences (Grant No: C2021329), the Key Disciplines Construction Project of Pudong Local Health Commission of Shanghai (Grant No: PWZxk2022-01), the Program for Outstanding Medical Academic Leader of Shanghai (Grant No: LJ202202), and the Shanghai Municipal Science and Technology Commission Project (Grant No: 22dz1202004). Dr. J.S. received grants from the Talent Development Program of Pudong Health Committee Shanghai (Grant No: PWRq2023-19), the Young Medical Talents Training Program of Pudong Hospital affiliated to Fudan University (Grant No: YQ202201), and the Scientific Research Foundation provided by Pudong Hospital affiliated to Fudan University (Grant No: YJYJRC202202). S.T. received grants from the Fudan Zhangjiang Institute Project (Grant No: KP7202109).
Author information
Authors and Affiliations
Contributions
K.J.S.K.: Data curation, Writing - Original draft preparation, Visualization; Investigation, Software, Methodology, Conceptualization; S.S.X.: Data curation, Methodology, Writing – Review & Editing; H.L.: Writing – Review & Editing, Methodology, Validation, Formal analysis; X.L: Writing – Review & Editing; Y.L.: Writing – Review & Editing, Software; B.C.: Writing – Review & Editing; S.T.: Writing – Review & Editing; H.Z.: Conceptualization, Methodology, Validation, Formal analysis, Resources, Data curation, Writing – Review & Editing, Supervision, Project administration; S.J.: Validation, Formal analysis, Resources, Supervision, Writing – Review & Editing, Project administration, Funding acquisition; J.D.T.: Supervision, Project administration, Writing – Review & Editing, Funding acquisition.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The UK Biobank has institutional review board approval from the Northwest Multicenter Research Ethics Committee, and all participants provided written informed consent. Secondary use of data for present analysis was approved by the Fudan University Pudong Medical Center Institutional Review Board.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article
Cite this article
Kwan, K.J.S., Xie, SS., Li, HL. et al. Evaluating the potential of phenotypic age to enhance cardiovascular risk prediction over chronological age in the UK Biobank. Sci Rep 15, 27858 (2025). https://doi.org/10.1038/s41598-025-12495-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12495-5

